Zerit
"Cheap 40 mg zerit with visa, medicine 75 yellow".
By: X. Folleck, M.A., M.D.
Associate Professor, Western Michigan University Homer Stryker M.D. School of Medicine
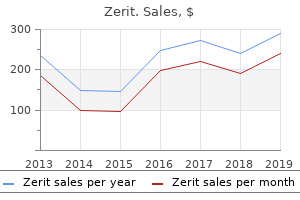
The available evidence symptoms 8dp5dt buy zerit 40 mg otc, consisting of large database analysis and population studies symptoms west nile virus cheap zerit 40mg on line, clearly show that low hemoglobin levels are associated with higher rates of hospitalizations medicine 19th century order zerit in united states online, cardiovascular disease treatment 9mm kidney stones purchase 40mg zerit mastercard, cognitive impairment, and other adverse patient outcomes, including mortality. Anemia in patients with chronic kidney disease is due to a number of factors, the most common of which is abnormally low erythropoietin levels. Other causes include: functional or absolute iron deficiency, blood loss (either occult or overt), the presence of uremic inhibitors (eg, parathyroid hormone, spermine, etc), reduced half life of circulating blood cells, deficiencies of folate or Vitamin B12, or some combination of these with a deficiency of erythropoietin. The causative role of erythropoietin deficiency in anemia of chronic kidney disease includes: (1) anemia is responsive to treatment with erythropoietin in all stages of chronic kidney disease; and (2) in patients with chronic kidney disease, circulating levels of erythropoietin are not sufficient to maintain hemoglobin within the normal range. North American (United States and Canada) and European studies have demonstrated these points. Studies reviewed for the purposes of this guideline include those of patients with chronic kidney disease prior to dialysis, those with kidney transplants, and those on dialysis. The reviewed literature spans almost 30 years of investigation and describes the clinical findings of researchers as they explore the relationships between hemoglobin and kidney function (Tables 76 and 77). The majority of available data have been derived from studies of small sample size, most of which are cross-sectional studies or baseline data from clinical trials of variable size and robustness. These studies are predominantly of only moderate or modest quality from a methodological standpoint. In 12 of the 22 studies reviewed, there was an association between the level of hemoglobin or hematocrit and the selected measure of kidney function. Published studies cited in Tables 76 and 77 demonstrate a variability in the levels of Fig 28. These data are based on the results of 446 patients enrolled in the Canadian Multicentre Longitudinal Cohort study of patients with chronic kidney disease. Erythropoietin levels in patients with chronic kidney disease have not been well characterized in studies to date and do not appear to be directly related to level of kidney function. The interpretation of these findings is that patients with kidney disease, as compared to normal individuals, do not have an appropriate rise in the levels of erythropoieten in the presence of anemia; while levels may be higher than non-anemic chronic kidney disease patients, the rise in erythropoietin levels is not commensurate with that seen in 142 Part 6. Table 77 shows the paucity of data in this area and the weakness of the association demonstrated by published studies between erythropoiten levels and level of kidney function. Several measures of iron stores have been studied in patients with kidney disease. Most of these measures, unlike bone marrow biopsy, do not directly quantify the amount of iron available for use in erythrocyte synthesis, relying instead on indirect or surrogate measures. Given the ``chronic inflammatory state' that may characterize chronic kidney disease, ferritin levels are not useful in measuring iron stores, nor in predicting the relation of hemoglobin to kidney function. Transferrin saturation, in combination with serum iron and ferritin levels, may be helpful in diagnosing functional iron deficiency-just as low serum ferritin levels are helpful in diagnosing iron deficiency anemia. Many of the published studies describe patients entered into clinical trials or seen by nephrologists. The reasons for these differences are incompletely studied but noted in conventional texts and review articles. Association 143 Interestingly, specific subgroups of patients (such as those with polycystic kidney disease) may have erythropoietin synthesis that is better preserved than other subgroups (such as diabetics). In the subgroup of patients who have kidney transplants, there are multiple causes for anemia in addition to decreased kidney function. The use of immunosuppressive agents or other medications, or chronic inflammation due to transplant rejection, may further confound the assessment of the etiology of declining hemoglobin. It is therefore difficult to determine whether the variability in hemoglobin at levels of kidney function is due to variability in measurements of kidney function or to variability associated with chronic kidney disease itself. While true variability between patients is the more likely possibility, the magnitude of variability is unknown. The issues of timing of intervention and specific target of hemoglobin are beyond the scope of this guideline. The characterization of severity of anemia for any individual with chronic kidney disease should be made in light of changes in hemoglobin from previous levels. Treatment and assessment recommendations are beyond the scope of this guideline 144 Part 6. For individuals who will not accept such a diet or who are unable to maintain adequate dietary energy intake with such a diet, an intake of up to 0.
Conversely medications used to treat anxiety order zerit 40mg free shipping, those with fewer years of education symptoms bladder cancer generic 40 mg zerit with amex, lower incomes medications blood donation order zerit online now, less accumulated wealth medications every 8 hours buy zerit 40mg overnight delivery, living in poorer neighborhoods, or substandard housing conditions have worse health outcomes. It is not only the abject lack of resources (income and assets) that contribute to health outcomes but also the income inequality in a community that predicts poorer health outcomes. Similarly, for most measures, racial and ethnic minorities have worse health outcomes than do whites. Many of the social factors that affect health have both independent and interactive effects. For example, people with higher incomes have more opportunities to live in safe and healthy homes, good communities, and near high quality schools. They are also generally better able to purchase healthy foods and afford time for physical activity. Health insurance and health care also become more accessible with more monetary resources. Conversely, people who are poor are more likely to live in substandard housing or in unsafe communities. Their communities may lack grocery stores that sell fresh fruits and vegetables or lack access to outdoor recreational facilities where they can exercise. Children who grow up in poverty generally fare worse in school and end up, on average, with fewer years of education than those in families with higher incomes. There is also a correlation between race/ethnicity and poverty, with racial and ethnic minorities more likely than whites to live in poverty. While many of these factors are interrelated, there is a growing body of literature that suggests some of these factors are also independent determinants of health. For example, in the United States health status for all racial and ethnic groups A a Low-income is defined as earning an income at or below 200% of the federal poverty guidelines, or $44,100/year for a family of four in 2009. Prevention for the Health of North Carolina: Prevention Action Plan 243 Chapter 11 Socioeconomic Determinants of Health People with higher incomes or personal wealth, more years of education, and who live in a healthy and safe environment have, on average, longer life expectancies and better overall health outcomes. Yet differences by income level and race/ethnicity remain even when taking the other into account. Other factors, including but not limited to , housing and education have similar independent and interactive affects on health. Research varies on which socioeconomic factor is the most important predictor of health. The Task Force did not attempt to try to answer which of these factors has the most important impact on health, recognizing that all of these factors should be addressed in order to improve the health of North Carolinians. In the United States, some people live, on average, 20 years less than others, depending on their race and/or ethnicity, socioeconomic status, or where they live. To improve population health, we need to improve the health of all of our residents, including racial and ethnic minorities, those living in poverty, or other marginalized or vulnerable populations. As the state moves forward to address the preventable risk factors discussed in this report, special attention should be focused on at-risk individuals and communities. Further it is important to also address socioeconomic risk factors directly, including strategies to reduce racial and ethnic disparities and poverty, and to increase decent affordable housing and improve educational outcomes for all North Carolinians. Identifying and creating policies and interventions aimed at reducing disparities-whether they are related to income, education, or race and ethnicity-will aid in improving the health of all North Carolinians. This chapter describes the interplay between socioeconomic factors and health in three areas: 1) poverty, wealth, and income inequality; 2) community and housing conditions; and 3) educational achievement. This link between b c 100% of the federal poverty guidelines is $22,050/year for a family of four in 2009. Based on percent of people in each income group reporting poor/fair health on the National Health Interview Survey, 2001-2006. Income, Wealth, and Income Inequality Income is positively related to health, with increasing income level corresponding to gains in health and health outcomes. Differences in income generally make the greatest difference for health at the lower end of the income scale; increases in income for the highest income groups may not produce significant gains in health. While the relationship between income and health has been shown across a range of health indicators, the association is not well understood. In addition, higher income individuals can more easily afford health insurance coverage.
Note: the data sources include population-based epidemiological studies medications j tube order zerit overnight delivery, disease registers treatment definition statistics buy zerit 40mg without prescription, and surveillance and notification systems medicine zetia purchase zerit 40 mg. Where possible medications known to cause pancreatitis buy 40 mg zerit mastercard, regional and global totals refer to numbers of separate studies, or country-years of reported data from surveillance or notification systems. As the table shows, more than 2,700 data sets contributed to the estimates for these 21 causes of death, with almost one-third of these relating to Sub-Saharan Africa. Since the original estimates for 1997 were completed, revised and updated estimates have been prepared. Trends in notification rates were assumed to represent trends in incidence rates for most countries except those with evidence of changes in case detection rates. China carried out a countrywide disease prevalence survey during 2000, and the results were used to reevaluate incidence for 1999. For other countries with evidence of changes in case detection rates, the trend for one of eight groups of epidemiologically similar countries was assumed to apply (Corbett and others 2003). For the most recent round of estimates, they used two different types of models depending on the nature of the epidemic in a particular country. For countries with epidemics concentrated in high-risk groups, they used prevalence estimates derived from the estimated population size and prevalence surveillance data in each high-risk category, and then employed simple models to back-calculate incidence and mortality based on these estimated prevalence trends (Stover and others 2002). For countries with usable death registration data, deaths due to diarrheal diseases were estimated directly from that data. For other countries, a regression model was used to estimate proportional mortality from diarrhea for children under five (Boschi-Pinto and others forthcoming). The regression data were drawn from more than 60 community-based studies carried out since 1980 with study durations of multiples of 12 months. This model was validated and supplemented with vital statistics from developing countries where coverage was high. In countries where routine vaccine coverage was low (less than 80 percent), incidence data were derived from a natural history model using country-specific vaccine coverage and attack rates from population-based studies (Crowcroft and others 2003). For countries with higher routine coverage and in the elimination phase, case notification and country-specific correction factors were used to estimate incidence. Pertussis cases and deaths were based on a natural history model using vaccine coverage and age-specific case fatality rates from community based studies, where available (Crowcroft and others 2003). The incidence estimates for polio and diphtheria (Stein 2002b; Stein and Robertson 2002) were based on countryspecific reported cases of acute flaccid paralysis with adjustments for underreporting and on country-specific notifications of diphtheria cases with an assumed notification efficiency of 20 percent, respectively. A case fatality rate of 10 percent was assumed for diphtheria in countries without high death registration coverage. Community-based studies with durations of one year or longer, published since 1980, were used to estimate the proportional mortality from acute respiratory infections in children under five in developing countries (Williams and others 2002). The results confirmed earlier findings that the proportion of deaths attributable to acute respiratory infections diminishes as general mortality diminishes. Much of the variability across studies in the proportion of child deaths attributed to acute respiratory infections was due to the use of verbal autopsies to determine the cause of death. Data from seven studies that compared verbal autopsies with hospital-based diagnoses indicated that the percentage of deaths due to acute respiratory infections could be underestimated by up to 4 percent. The modeled estimates were supplemented with vital statistics from developing countries where coverage was high to develop regional and global estimates. The Burden of Disease and Mortality by Condition: Data, Methods, and Results for 2001 63 Malaria. Malaria mortality estimates for all regions except Sub-Saharan Africa were derived from the cause of death data sources described earlier. For Sub-Saharan Africa, country-specific estimates of malaria mortality were based on analyses by Snow and others (1999) and updated using the most recent geographical distributions of risks from the Mapping Malaria Risks in Africa International Collaboration. These estimates were supplemented with and validated against vital statistics from Latin American countries where coverage was high. For countries without death registration data, both nationally reported data and specific criteria for a regression model were used to estimate maternal mortality. Deaths from these causes, primarily low birthweight, prematurity, and birth trauma or asphyxia, may occur at any age, and can include some maternal or placental causes, such as multiple pregnancy. Deaths from these causes should not be confused with deaths that occur during the perinatal period, which include stillbirths and neonatal deaths from other causes such as tetanus and congenital malformations. However, acknowledging that nearly all deaths due to perinatal causes occur during the neonatal period, we first estimated the envelope of neonatal mortality for every country (for details of the method see Murray and Lopez 1998). This age-period-cohort model of cancer survival was based on data from the Surveillance, Epidemiology, and End Results program of the National Cancer Institute (Ries and others 2002).

Such a result indicates that the observed result would be highly unlikely under the null hypothesis symptoms uterine prolapse order zerit 40mg online. Research and statistics: case reports administering medications 7th edition best zerit 40mg, anecdotal evidence symptoms breast cancer order zerit with a mastercard, and descriptive epidemiologic studies in pediatric practice symptoms 3dpo cost of zerit. Radiological findings: Lateral soft tissue X-ray examination of the neck demonstrates enlargement of the adenoids (star), enlarged lingual tonsils at the base of the tongue (big arrow), and narrowing of the nasopharyngeal airway (small arrow). Final diagnosis: Traumatic fracture in the right parietal bone complicated by an intracranial epidural hemorrhage and cephalhematoma. Radiological findings: Skull X-ray images show a premature closure of the anterior part of metopic suture, which runs from the top of the head at the anterior fontanel, resulting in deformation of the anterior portion of the calvarium and a triangular-shaped forehead (trigonocephaly). Case 4 A 2-year-old boy has fever, sore throat, dysphagia, and neck pain for 1 week. Multiple bilateral frontal and orbital fractures with air in the brain can be seen (images B and C). The 3-D reconstructed image revealed bilateral frontal fractures (arrows in image C). Radiology Review 549 Case 6 Case 7 A 15-year-old boy with a history of travel to South America presented with muscular pain, severe headache, and recurrent seizures. Note: Neuroblastoma is the third most common malignant neoplasm of childhood, after leukemia and brain tumors. Case 10 A premature baby presented with sudden unexplained drop in hematocrit levels, a transfontanelle ultrasonography ordered immediately. Radiological findings: Extensive intraventricular hemorrhage (coronal and sagittal) with extension to the brain tissues around the right lateral ventricles (arrows). Clinical examination showed papilledema and A 10-year-old boy is presented with two months history of headaches, a recent history of vomiting and ataxia. Case 13 A 2-year-old girl is presented with 10 days history of lowgrade fever, runny nose, and discharge in both ears. Final diagnosis: Bilateral sinusitis, otitis media, and mastoiditis complicated by a left subperiosteal abscess. Case 12 A 5-year-old girl presented with short neck, low hairline at the back of the head, and restricted mobility of the upper spine along with standing torticollis. Radiological findings: Lateral X-ray view of cervical spine showing fusion of cervical vertebrae and tracheal deviation to the left side (arrow on images A and B). Radiological findings: Transfontanelle ultrasonography shows periventricular calcifications (big arrows on image 552 A. Notes: Brainstem gliomas are the most common brain tumors in children between 7 and 9 years of age. They account for approximately 25 % of all posterior fossa tumors without any gender or racial predilection. Radiological findings: Depressed skull fracture in the left parietal bone (arrows on images A, B, and C) without any associated intracranial hemorrhage. Case 15 A 13-year-old boy presented with a history of long-standing headache and frequent seizures. A 10-year-old boy presented with a history of progressive headache, abnormal gait, and visual problems. Radiology Review 553 Case 17 Case 18 A 4-year-old girl presented with growth retardation and polyurea. Image C: T1 C + (Gd) shows cystic hypointense lesion without contrast enhancement; however, a thin enhancing rim of surrounding compressed pituitary tissue may be seen. A 3-month-old boy presented with high fever, vomiting, poor feeding, and bulging anterior fontanelle. Case 19 the densities become coalescent in many areas and heart borders are completely obliterated (image B). Note the malposition of the endotracheal tube (small arrow in image A) and thorax drain for pneumothorax (big arrow on image A). Case 21 A 1-day-old newborn boy presented with cyanosis, which improves when he cries.
Purchase zerit 40mg free shipping. Dehydration | Dehydration in malayalam.