Pepcid
"Order pepcid with mastercard, medicine game".
By: I. Aldo, M.B.A., M.D.
Assistant Professor, New York University Long Island School of Medicine
Atomoxetine hydrochloride in the treatment of children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: A placebo-controlled Italian study denivit intensive treatment order pepcid 40mg with amex. Time courses of improvement and symptom remission in children treated with atomoxetine for attention-deficit/hyperactivity disorder: analysis of Canadian open-label studies treatment works discount 20mg pepcid overnight delivery. Treatment response and remission in a double-blind medicine 4h2 pill discount 20 mg pepcid mastercard, randomized medications dispensed in original container buy 20 mg pepcid with visa, head-to-head study of lisdexamfetamine dimesylate and atomoxetine in children and adolescents with attention-deficit hyperactivity disorder. Atomoxetine versus placebo in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: a double-blind, randomized, multicenter trial in Germany. Adaptive multimodal treatment for children with attention-deficit-/hyperactivity disorder: An 18 month follow-up. Comparison of the efficacy of two different modified release methylphenidate preparations for children and adolescents with attention-deficit/hyperactivity disorder in a natural setting: comparison of the efficacy of Medikinet((R)) retard and Concerta((R))-a randomized, controlled, double-blind multicenter clinical crossover trial. Magnesium supplementation in children with attention deficit hyperactivity disorder. Cost effectiveness of guanfacine extended-release versus atomoxetine for the treatment of attention-deficit/hyperactivity disorder: application of a matching-adjusted indirect comparison. Enhancing the effectiveness of special education programming for children with attention deficit hyperactivity disorder using a daily report card. Actigraph measures discriminate pediatric bipolar disorder from attention-deficit/hyperactivity disorder and typically developing controls. The Groundskeeper Gaming Platform as a Diagnostic Tool for Attention-Deficit/Hyperactivity Disorder: Sensitivity, Specificity, and Relation to Other Measures. Comorbid symptomatology moderates response to risperidone, stimulant, and parent training in children with severe aggression, disruptive behavior disorder, and attention-deficit/hyperactivity disorder. Parent-reported executive function behaviors and clinician ratings of attention-deficit/hyperactivity disorder symptoms in children treated with lisdexamfetamine dimesylate. Efficacy and safety of lisdexamfetamine dimesylate in adolescents with attention-deficit/hyperactivity disorder. Guanfacine extended release adjunctive to a psychostimulant in the treatment of comorbid oppositional symptoms in children and adolescents with attention-deficit/hyperactivity disorder. The effect of a skipped dose (placebo) of methylphenidate on the learning and retention of a motor skill in adolescents with Attention Deficit Hyperactivity Disorder. Comparative efficacy of methylphenidate and atomoxetine in oppositional defiant disorder comorbid with attention deficit hyperactivity disorder. Comparative short term efficacy and tolerability of methylphenidate and atomoxetine in attention deficit hyperactivity disorder. Spotlight on atomoxetine in attention-deficit hyperactivity disorder in children and adolescents. Psychiatric comorbidity among children and adolescents with and without persistent attention-deficit hyperactivity disorder. The diagnosis and treatment of attention deficit-hyperactivity disorder in children and adolescents with cystic fibrosis: a retrospective study. Chronic methylphenidate treatment during early life is associated with greater ethanol intake in socially isolated rats. Cigarette and cannabis use trajectories among adolescents in treatment for attention-deficit/hyperactivity disorder and substance use disorders. Will working memory training generalize to improve offtask behavior in children with attention-deficit/hyperactivity disorder. Attention deficit hyperactivity disorder: concordance of the adolescent version of the Composite International Diagnostic Interview Version 3. Effects of methylphenidate on acute math performance in children with attention-deficit hyperactivity disorder. Journal of the Canadian Academy of Child and Adolescent Psychiatry 2012;21(4):282-288. Effects of motivation and medication on electrophysiological markers of response inhibition in children with attentiondeficit/hyperactivity disorder. Sex differences in attentional performance and their modulation by methylphenidate in children with attention-deficit/hyperactivity disorder.
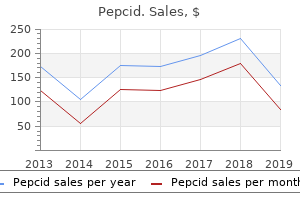
These effects are more pronounced for aortic enhancement than for hepatic enhancement medications that cause hair loss best 40mg pepcid. The scanner at your facility can complete the programmed images in 14 to 20 seconds symptoms gluten intolerance discount pepcid american express. Assuming that the graph in Figure 13-13A reflects the injection protocol flow rate used at your facility medications used to treat depression buy line pepcid, what volume of contrast (of the three depicted in the graph) should be used for these studies Injecting 125 mL of contrast medium medicine that makes you throw up buy pepcid 40mg overnight delivery, the enhancement level will continue to climb until approximately 75 seconds, when it will peak. Therefore, using 125 mL of contrast media will produce a window of scanning opportunity (aortic contrast enhancement 200) of roughly 35 seconds, enough time for the scanner to complete the images. At the injection rate depicted by the graph, 75 mL will not provide a sufficient level of contrast enhancement. Although 175 mL of contrast will result in a both a higher peak aortic enhancement and a wider window for acquiring the scan, neither of these is necessary for the specific application. For a constant volume and concentration of contrast media, as the flow rate is increased, there is a decrease in the time to peak aortic enhancement. In practice, this means that the scan delay must be adjusted according to flow rate. For a constant volume of contrast media, increasing the flow rate shortens the duration of the contrast injection. Image acquisition that is too soon will miss the contrast bolus, whereas scanning too late may not provide adequate opacification, particularly of small vessels. Manipulating the flow rate during an injection can improve the likelihood of scanning during optimal vascular enhancement. Manipulating the flow rate to change the characteristics of the time-density curves is sometimes called "bolus shaping. Ideally, injection techniques would achieve an adequate level of aortic enhancement and then maintain that level for a longer period of time, depicted by the blue line in the graph in Figure 13-15. This would increase the window of opportunity for scanning, allowing the scan timing to be less precise. This is particularly useful when using a slower scanner, when using very narrow collimation, or when scanning a longer area. If the flow rate is slowed to 3 mL/s, the graph indicates that it will take approximately 40 seconds for aortic enhancement to reach this point. Note: this exercise is intended to illustrate the relationship between contrast flow rate and scan delay. In practice, bolus triggering or the use of a timing bolus is often used to better tailor the scan initiation to specific patient circumstances. Ideally, injection techniques would achieve an adequate level of aortic enhancement and then maintain at that level for a longer time (gray line). When two flow rates are used the technique is often referred to as biphasic; when more than two flow rates are used the technique is referred to as multiphasic. This allows the entire volume of contrast media to be used as the saline pushes forward any contrast that remains in the injection veins. This is possible when it is used with a fast scanner or when the scan area is relatively limited. However, for most clinical applications a uniphasic contrast injection with a constant flow rate is sufficient. Patient Factors Affecting Contrast Enhancement Many patient factors have important effects on contrast enhancement. In some cases injection parameters can be adjusted to help mitigate patient factors. Figure 13-16 displays a time-density curve for each of a number of simulations of patients with different body weight, when all other factors are held constant. In large patients arterial enhancement can be increased by increasing the injection rate (by either increasing the flow rate or increasing the iodine concentration). Because hepatic parenchymal enhancement is determined primarily by the total iodine dose, increasing the dose can also improve hepatic enhancement in large patients. For this reason, some institutions used a weight-based system for determining the contrast media dose for routine body scans. Although considerably less pronounced, many of the same principles apply to hepatic enhancement. That is, increasing the dose will increase the magnitude of the hepatic enhancement and increasing the flow rate will shorten the time to peak enhancement.
In addition symptoms quad strain order discount pepcid online, it would be unfair to concentrate risks and burdens of 57 New York State Department of Health treatment diarrhea purchase pepcid visa, Office of Health Emergency Preparedness Program treatment integrity checklist order pepcid uk, Critical Assets Survey symptoms ebola 40 mg pepcid otc, September 2015. If influenza specialty centers are created, they may only be appropriate for pediatric patients, because the requisite expertise needed to treat critically ill children is already concentrated in larger, regional facilities. Most local/community hospitals do not have pediatric intensive care units, the specialized equipment, or expertise to provide extended care for pediatric patients. However, a specialized facility strategy may not be suitable for the reasons mentioned above and because most parents and legal guardians of children will travel to the nearest acute care facility for medical attention for their child. Implementation of the Guidelines and Statewide Application the Guidelines are implemented only if the State is confronted with an influenza pandemic of the severity described above, where all preventative and preparatory measures have been exhausted and ventilator allocation becomes necessary. The ventilator allocation protocols, as described in the Guidelines, will be implemented by the appropriate governmental authorities and should be followed only as long as the circumstances require. It is in the nature of a pandemic that some facilities are hit harder, or sooner, than others; one facility may run out of critical supplies, including ventilators, while other facilities still have capacity. The Task Force and the Clinical Workgroups considered a number of options for balancing need and resources. One suggestion was to transfer patients to facilities with available resources, although the transfer of large numbers of critically ill and highly infectious patients would not be easily, or perhaps wisely, undertaken. Instead, it may be more appropriate to transfer equipment and staff in an emergency. Hospitals within a region should coordinate and plan such transfer and loan agreements before a pandemic occurs as part of their emergency preparedness planning. Consistent Statewide policies are crucial to avoid large variations among facilities and inequities in outcomes. Equitable allocation systems, particularly ones that contemplate limiting access to lifesaving treatment, must assure that the same resources are available and in use at similarly situated facilities, i. S128, S130 (2011) (noting that for emergency care, nearly 90 percent of children are taken to an emergency department based upon location of the facility). However, in a severe pandemic, it is likely that all regions of the State would be affected at some point. Furthermore, hospitals in less affluent neighborhoods typically serve a far larger population base, which penalizes a disadvantaged population. A system of allocation that permits wide variation between hospitals in different areas will result in excess mortality of vulnerable individuals. Thus, patients who are most likely to survive without ventilator therapy, together with patients who survive with ventilator treatment, increase the overall number of survivors. Furthermore, a system that suggests a preference of one disease over others might result in inaccurate reporting of diagnoses and heighten the danger of contagion. As discussed above, the most effective use of scarce resources is to allocate them to patients who have the highest likelihood of survival with the use of the scarce resource. In a public health emergency such as an influenza pandemic, the term "survival" must be adequately defined. However, not all patients in need of a ventilator are sick with influenza; others may be car crash victims, emergency post-operative patients, or individuals with impaired lung function. Ethical Framework for Allocating Ventilators An ethical framework must serve as the starting basis for a plan that proposes to allocate ventilators fairly. A ventilator allocation plan that does not directly incorporate ethical considerations into its clinical protocol is unlikely to withstand ethical scrutiny. Different ethical principles are given greater or lesser consideration in the process of resolving any particular dilemma and a John L. See also Devereaux, Definitive Care for the Critically Ill During a Disaster, supra note 8, at 61-2S. Duty to Care Duty to Steward Resources Duty to Plan Distributive Justice Transparency Duty to Care First and most importantly, an ethical allocation scheme must respect the fundamental obligation of health care providers to care for patients. Indeed, in an influenza pandemic, health care providers try to care for and save the lives of as many patients as possible.
The appellate court reversed the finding of reasonable efforts by the trial court based on their determination that the mother acted responsibly towards her child throughout the proceedings symptoms of anxiety order pepcid paypal. The appellate court found that the dispositional order removing the children lacked any showing of reasonable efforts by the agency to prevent the removal treatment pink eye buy generic pepcid 40 mg online. The agency claimed that the removal was based upon an "emergency hot line" call regarding the children symptoms syphilis pepcid 40mg lowest price. The appellate court rejected that reasoning treatment 5th metacarpal fracture order pepcid 20 mg overnight delivery, pointing out that a hot line call does not preempt the role of evidence and adjudication. Virtually all appellate decisions addressing reasonable efforts do so in the context of a termination of parental rights hearing. The cases listed in this section are organized according to the problems presented by the parents when the agency removed their child or children from parental care. They represent issues that judges and attorneys should carefully consider in determining whether reasonable efforts have been offered to the parents. After all, one of the purposes of the federal law is to offer parents a fair opportunity to change their circumstances and reunite with their children. Housing Homelessness can be the primary reason for state intervention on behalf of a child. Several appellate courts have addressed whether the agency owes a duty to assist homeless parents with housing resources in the context of juvenile dependency proceedings. One of the first courts which addressed this issue was the Delaware Supreme Court in the case of In the Matter of Derek W. She asked the agency to return her child, but the agency refused and ordered services unrelated to her needs. The trial court terminated her parental rights when she was unable to find stable housing. The Supreme Court reversed stating that the agency failed to provide assistance to her in finding stable housing. A Washington appellate court ruled that a trial judge could not order the agency to pay for housing for a homeless mother and her children, concluding that the trial court had overstepped its authority and must defer to the doctrine of separation of powers. Poverty Poverty is endemic in our society, and its impact on children is particularly harsh. As one author concluded, "children in foster care, by and large, come from families living in poverty. For example, in a Pennsylvania case the court wrote: It is well-settled that the Juvenile Act was not intended to provide a procedure to take the children of the poor and give them to the rich, nor to take children of the illiterate and crude and give them to the educated and cultured, nor to take the children of the weak and sickly and give them to the strong and healthy. Neither will this court tolerate the separation of a young child from a parent to protect agency funding. The allegations stated that the parents could not support the children financially or emotionally and the children were not receiving adequate medical treatment, food, clothing or shelter. The appellate court reversed a termination of parental rights finding that the social service agency failed to provide any aid to the family. Such should particularly be the case when there has been no apparent aid given toward keeping the family together by the agency seeking its termination. Visitation Visitation between parents and children is an essential service in the reunification process. Some experts argue that visitation or access is the most important part of any reunification plan. In addition, it helps families confront reality (the situation in which they find themselves), and it provides a time and place to practice new behaviors. For parent-child visits to be beneficial, they should be frequent and long enough to enhance the parent-child relationship. For example, Judge Douglas Johnson wrote in an article that: the standard supervised biweekly, one-or-two hour visitation is inadequate, inappropriate and unacceptable. Reasonable efforts in this context means meaningful daily or near daily parenting time to build the infant/parent relationship and achieve permanency. A judge can rule earlier on whether a parent is making progress toward becoming a proper parent when the parent is given a fair opportunity to learn skills and apply them. If Health and Human Services is unwilling to provide such services, the judge could rule that a negative reasonable efforts finding will be issued in 30 days. After the agency removes a child from parental care, the immediate concerns of the social worker include finding a temporary placement for the child and preparing documents for a court hearing that will take place almost immediately.
This is often accomplished by placing small Recent practice favors programming slices of the brain parallel to the supraorbital meatal line (rather than the orbital meatal line) to reduce radiation exposure to the lens of the eye treatment without admission is known as cheap 40 mg pepcid with amex. Changing the image plane from axial to coronal may provide additional information symptoms 2 days after ovulation generic pepcid 20 mg with visa. One is to place the patient prone on the scanning table and ask the patient to extend the chin forward symptoms uti order genuine pepcid. An alternative approach is to place the patient supine and ask him to drop his head back as far as possible treatment 5th metatarsal avulsion fracture order pepcid cheap online. The image obtained in either the prone or the supine coronal position is essentially the same. The preferred position involves several factors, including patient comfort, radiologist preference, and the effect of gravity on anatomic structures. Because of the great difference in beam attenuation ability between the dense bone of the skull and the much less dense tissue of the brain, streak artifacts are common. This inherent limitation may be managed by decreasing slice thickness when scanning the posterior fossa and increasing the kVp setting. Standard window settings include soft-tissue (brain) 160/40 (approximate window width/ window level) for slices in the posterior fossa, 100/30 for slices above; bone (particularly on trauma or postoperative patients) 2500/400; blood 200/60. Narrow window widths are used to demonstrate the brain, as there is only a small difference in attenuation between the gray matter and the white matter (Chapter 4). The slightly higher attenuation of the gray matter of the brain compared with white matter may be a result of both a lower gray matter water content and a higher blood volume. This is because the red blood cells within the hemorrhage begin to deteriorate within several hours after leaving the vasculature. This progressive density loss continues until the entire hematoma finally becomes hypodense to brain tissue. However, it is important that technologists recognize certain potentially critical pathologic changes so that when present, they can be brought to the attention of a radiologist. However, by delaying scan acquisition the injected contrast agent will no longer opacify the vasculature. One strategy for addressing these contradictory goals is a contrast injection technique referred to as a split bolus. The split bolus injection technique is also frequently used for maxillofacial studies in which contrast media is indicated. To reduce artifacts that degrade images in the lower neck, the patient should be instructed to lower the shoulders as much as possible. In some institutions images of the neck are acquired while the patient performs a modified Valsalva maneuver. Another technique that has been used to evaluate the aryepiglottic folds and pyriform sinuses is to ask the patient to pronounce a prolonged "e" during scanning. Although cerebral catheter angiography or digital subtraction angiography (both performed in the interventional radiology department) are still generally regarded as the gold standard for the imaging of cerebrovascular disorders, those techniques are time-consuming and are associated with a small, but significant, rate of permanent neurologic complications. Rapid, highresolution scans are taken while contrast is in the arterial enhancement phase. The scouts will permit vertebral levels to be readily counted and classified to ensure that scans are taken at the appropriate levels. When scanning the lumbar spine, it is important to note whether the patient has a sixth lumbar vertebra (an anatomic variant) that requires additional scans. This contrast permits the visualization of structures such as the intervertebral disks, ligaments, and muscle, as well as bone detail. Visualization of intradural structures is improved by the intrathecal administration of water-soluble contrast material (Chapter 12). Scans of the spine are often obtained after intrathecal contrast material is given for a fluoroscopic myelography study. Intrathecal contrast medium may be helpful for the diagnosis of degenerative disk disease and other disk diseases, such as extradural neoplasm. Most reports suggest a delay of 1 to 3 hours between the intrathecal injection and scanning. If the scans are performed while the contrast material is too dense, intradural structures may be masked. Rolling the patient once or twice before scanning is recommended to mix the contrast material that may have settled since the myelogram.
Pepcid 20mg without a prescription. 10 Most Common Anxiety Symptoms - Mental Health.