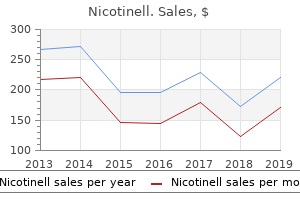
Nicotinell
"Buy nicotinell from india, quit smoking brochures".
By: C. Zapotek, M.B.A., M.B.B.S., M.H.S.
Clinical Director, TCU and UNTHSC School of Medicine
Use with caution in patients with a history of syncope quit smoking 3 months ago and still tired all the time buy nicotinell without prescription, in patients receiving concomitant medications that may cause hypotension quit smoking with hypnosis discount generic nicotinell canada, and in patients who are dehydrated quit smoking 45 days buy discount nicotinell 52.5 mg online. Patients may present with blindness quit smoking prescription buy nicotinell without a prescription, confusion, headache, hypertension, lethargy, seizure, or other visual or neurologic disturbances. Use caution in patients who are receiving multiple concomitant medications and/or who have serious underlying medical conditions; asymptomatic increases in liver enzymes, hyperbilirubinemia, hepatitis, and rare cases of acute liver failure have been reported. Incidence may be increased in patients treated previously with neurotoxic agents. Improvement in or a resolution of peripheral neuropathy has been reported following dose adjustment or discontinuation of bortezomib. Allopurinol and/or alkalinization of the urine may be indicated for serious tumor lysis syndrome. Monitor blood glucose levels and adjust antidiabetic medications as indicated; see Drug/ Lab Interactions. Should pregnancy occur, notify physician immediately and discuss potential hazards. Elderly: Safety and effectiveness similar to other age-groups; however, greater sensitivity in the elderly cannot be ruled out. In clinical trials, patients over 65 years of age had a slightly increased incidence of Grade 3 or 4 toxicity. Other examples of inhibitors may include cimetidine (Tagamet), erythromycins, grapefruit juice, antifungal agents. Inducers may increase metabolism and decrease serum levels and effectiveness of bortezomib. Examples of inducers may include carbamazepine (Tegretol), phenobarbital (Luminal), phenytoin (Dilantin), rifampin (Rifadin). Some examples are acyclovir (Zovirax), amiodarone (Nexterone), antineoplastics. Monitor blood glucose levels and adjust dose of antidiabetic medication as indicated. Most common side effects reported include anemia, anorexia, constipation, diarrhea, fatigue, fever, leukopenia, lymphopenia, nausea and vomiting, neuralgia, neutropenia, peripheral neuropathy, rash, and thrombocytopenia. Abdominal pain, arthralgia, asthenia, bronchitis, chills, cough, dehydration, dizziness, dysesthesia, edema, headache, hypertension, malaise, nasopharyngitis, paresthesia, peripheral edema, pneumonia, psychotic disorders. Overdose: Profound progressive hypotension, tachycardia, and decreased cardiac contractility. Symptomatic hypotension and thrombocytopenia with fatal outcomes have been reported in patients who received more than twice the recommended dose. Temporarily discontinue bortezomib if Grade 4 thrombocytopenia occurs (less than 25,000/mm3); may be resumed at a reduced dose after thrombocytopenia is resolved. Symptoms of peripheral neuropathy may improve or return to baseline if bortezomib is discontinued. Hypotension may respond to adjustment of antihypertensive medications, hydration, or administration of mineralocorticoids. For new or worsening cardiopulmonary symptoms, consider interrupting bortezomib until a prompt and comprehensive diagnostic evaluation is conducted. For symptoms of serious liver dysfunction, interrupt bortezomib to assess reversibility. There is no specific antidote; supportive therapy will help sustain the patient in toxicity. To hasten the dissolution, release the residual vacuum after the water is transferred into the evacuated vial. Infusion should begin within 2 hours of reconstitution and should be completed within 4 hours of reconstitution. Filter: Use of an in-line or syringe-tip, sterile, disposable filter (18 micron) is recommended. If a pre-existing line must be used, botulism immune globulin should not be diluted more than 1:2 with any of the previously named solutions. If no untoward reactions after 15 minutes, the rate may be increased to 1 mL/kg/hr (50 mg/kg/hr) for the remainder of the infusion. A specialty immunoglobulin (IgG) containing neutralizing antibodies to botulinum toxin types A and B. Should provide the relevant antibodies at levels sufficient to neutralize the expected levels of circulating neurotoxins in infants who may have been exposed to botulinum toxin types A or B.
Pharmacoeconomics: Not only the poor countries but even the rich nations are now finding it difficult to control the ever-rising cost of medical care quit smoking 40 days ago buy discount nicotinell 35 mg. For several decades quit smoking coupons cheap 35mg nicotinell with mastercard, this book has been consistently emphasising that while selecting a drug quit smoking 30 days cheap nicotinell 35 mg free shipping, its cost-effectiveness (getting the maximum benefit at the minimal cost) and cost-benefit ratio should be taken into consideration quit smoking 48 hours purchase 52.5mg nicotinell with visa. How many practitioners know that the cost of the same drug promoted under different brand names may vary as much as 5-10 times? Dermal preparations containing the newer potent steroids are far more expensive than equally effective, well established, older preparations. This approach will help more prudent deployment of the available resources for better medical care in the society at large. Patient compliance: Except when hospitalised, patients are responsible for taking their own drugs. Often, there is a discrepancy between what is prescribed and what the patient actually takes. The drug regimen should be as simple as it can be kept: as few drugs as possible and once or twice a day administration, if permissible. A sympathetic discussion about the difficulties of drugs prescribed and about the possible adverse effects is likely to have a salutary effect on compliance. On the other hand, mere distribution of printed leaflets about drugs prescribed, diet etc, may educate the patient but is less effective in improving patient compliance. Although, a surprise check on urine or plasma level of the drug or its metabolite helps to detect defaulters, it may be impracticable. For example: cephalosporins of the first generations are (among cephalosporins) the preferred drugs in Gram positive infections. Drugs expiry date: Do the drugs become useless after the expiry date mentioned by the manufacturers? Drug companies, because of certain legal compulsions and liability concerns, will not advocate such use after the expiry date mentioned on the package which is usually 2-3 years from the date of manufacture. Shelf-life of a drug is the time where a given product, stored under reasonable conditions, is expected to remain stable (> 90% of potency). According to Medical Letter (Volume 44, 93, 2002), "There are virtually no reports of toxicity from degradation products of outdated drugs (except tetracycline). How much of their potency they retain varies with the drug and the storage conditions, especially humidity but many drugs stored under reasonable conditions retain 90% of their potency, for at least 5 years after the expiration date on the label, and sometimes much longer ". In some countries, counterfeit medicines may constitute 20-50% of the available products. They may comprise low quality manufacture of correct ingredients; wrong/undisclosed ingredients; adulteration; insufficient quantity of ingredients; false labelling; or no active ingredient at all. Examples are glucocorticoids added to herbal medicines for asthma and arthritis; and turmeric dispensed as tetracycline. For detection of counterfeit drugs, one needs a good infrastructure for vigilance and for enforcement of drug regulations. P-drug (Personal drug) Concept In practice, the physician usually needs 50-60 drugs routinely to treat common ailments. Pdrugs are the drugs one chooses for prescribing regularly and with which one becomes familiar. Such a list would spare the physician repeated search for a better drug from among the many available. Many patients may have to be treated with a less-than-ideal drug which has to be accepted because of the unaffordable cost or non-availability of the ideal drug. They should, therefore, be available at all times in adequate amounts and in appropriate dosage forms, at a price the individual and the community can afford. The section on reserve antiinfective agents could thus be integrated into the complementary list.
Cervical cancer Squamous cell carcinoma Contraindications Hypersensitivity to drug or other platinum-containing compounds Severe impairment of renal function Severe myelosuppression Hearing impairment Pregnancy or breastfeeding Precautions Use cautiously in: mild to moderate renal impairment quit smoking 6th day purchase 17.5mg nicotinell otc, active infection quit smoking 8 months ago generic nicotinell 17.5mg, myelosuppression quit smoking 3 months ago women order nicotinell 35 mg with visa, chronic debilitating illness quit smoking 5 as discount nicotinell online amex, heart failure, electrolyte abnormalities females of childbearing age. In well-hydrated patients with good renal function, infusions of 100 to 500 ml may be given over 30 minutes. Monitor neurologic status, hepatic enzyme and uric acid levels, and audiogram results. Onset Unknown Peak 18-23 days Duration 39 days Patient teaching Instruct patient to drink 8 oz of water every hour while awake. Amphotericin B, loop diuretics: increased risk of hypokalemia and hypomagnesemia Antineoplastics: additive bone marrow depression Live-virus vaccines: decreased antibody response to vaccine, increased risk of adverse reactions Nephrotoxic drugs (such as aminoglycosides): additive nephrotoxicity Ototoxic drugs (such as loop diuretics): additive ototoxicity Phenytoin: reduced phenytoin blood level citalopram hydrobromide Celexa Pharmacologic class: Selective serotonin reuptake inhibitor Therapeutic class: Antidepressant Pregnancy risk category C Reactions in bold are life-threatening. Dosage adjustment 1Indications and dosages Hepatic impairment Elderly patients Alcoholism Panic disorder Premenstrual dysphoria Social phobia Off-label uses Interactions Drug-drug. Availability Granules for oral suspension: 125 mg/ 5 ml, 250 mg/5 ml Tablets: 250 mg, 500 mg Tablets (extended-release): 500 mg Patient teaching Instruct patient to take drug with full glass of water at same time every day. Instruct patient to move slowly when sitting up or standing, to avoid dizziness or light-headedness caused by sudden blood pressure decrease. As appropriate, review all other significant and life-threatening adverse Pharyngitis or tonsillitis caused by Streptococcus pyogenes Adults: 250 mg P. Administration Obtain specimens for culture and sensitivity testing as appropriate before starting therapy. Patient teaching Advise patient to take drug with full glass of water, either with food or on an empty stomach. Tell patient using oral suspension not to refrigerate it, and to discard it 14 days after mixing. Consider this diagnosis in patients who develop diarrhea after drug administration. If diagnosis of pseudomembranous colitis has been established, initiate therapeutic measures. In moderate to severe cases, consider giving fluids and electrolytes, protein supplements, and antibacterial drug effective against Clostridium difficile colitis. Diarrhea, colitis, and pseudomembranous colitis may first appear up to several weeks after clindamycin therapy ends. Reserve drug for serious infections when less toxic antimicrobials are inappropriate. Severe infections caused by sensitive organisms (such as Bacteroides fragilis, Clostridium perfringens, Fusobacterium, pneumococci, staphylococci, and streptococci) Adults: 300 to 450 mg P. Topical, vaginal Onset Rapid Rapid Rapid Peak 45 min End of infusion 1-3 hr Duration 6-8 hr 6-8 hr 6-8 hr Children: 16 to 20 mg/kg/day P. Alanine aminotransferase, alkaline phosphatase, aspartate aminotransferase, bilirubin, creatine kinase: increased levels Platelets, white blood cells: transient decrease in counts Contraindications Hypersensitivity to drug or lincomycin Precautions Use cautiously in: renal or hepatic impairment known alcohol intolerance pregnant patients neonates. Patient monitoring Monitor creatinine level closely in patients with renal insufficiency. Assess for signs and symptoms of hypersensitivity reactions, including anaphylaxis. Caution patient not to rely on condoms or diaphragm for contraception for 72 hours after using vaginal preparation; drug may weaken latex products and cause breakage. Availability Solution for injection: 1 mg/ml (20 mg in 20-ml flint vials) c Relapsed or refractory acute lymphoblastic leukemia after at least two previous regimens Children and adults ages 1 to 21: 52 mg/m2/day by I. Resulting admixture may be stored at room temperature but must be used within 24 hours of preparation. If early signs or symptoms of these life-threatening syndromes occur, stop drug immediately and start appropriate supportive measures. If hypotension is transient and resolves without pharmacologic intervention, reinstitute drug (generally at lower dosage). Drug may be reinstituted (possibly at lower dosage) when patient is stable and organ function returns to baseline. Know that after recovery or return to baseline organ function, treatment cycles are repeated about every 2 to 6 weeks. Dosage is based on body surface area, calculated using actual height and weight before start of each cycle. Avoid concurrent administration of hepatotoxic or renotoxic drugs during 5 days of treatment. Onset Unknown Peak Unknown Duration Unknown Hepatic: hepatomegaly, jaundice Musculoskeletal: arthralgia, back pain, myalgia, limb pain Respiratory: pneumonia, cough, dyspnea, pleural effusion, respiratory distress Skin: contusion, dermatitis, herpes simplex, dry skin, erythema, palmarplantar erythrodysesthesia, petechiae, pruritus, cellulitis Other: decreased appetite, weight loss, edema, injection site pain, mucosal inflammation, pain, fever, bacteremia, sepsis, staphylococcal infection, transfusion reaction Interactions Drug-drug.
Thus quit smoking ear treatment order 17.5 mg nicotinell with visa, during periods of stress quit smoking zinnone discount nicotinell 52.5mg otc, trauma quit smoking using hypnosis buy nicotinell us, or severe exercise quit smoking vietnam cheap nicotinell line, the elevated epinephrine levels can override the effect on the cell of circulating substrates. In these situations-regardless of the concentration of blood glucose-glucagon levels are elevated in anticipation of increased glucose use. Both substances are increased following ingestion of glucose or a carbohydrate-rich meal (see Figure 23. Effects on carbohydrate metabolism: the intravenous administra- tion of glucagon leads to an immediate rise in blood glucose. This results from an increase in the breakdown of liver (not muscle) glycogen and an increase in gluconeogenesis. The free fatty acids released are taken up by liver and oxidized to acetyl coenzyme A, which is used in ketone body synthesis. Mechanism of action of glucagon Glucagon binds to high-affinity G protein-coupled receptors on the cell membrane of hepatocytes. The receptors for glucagon are distinct from those that bind insulin or epinephrine. This cascade of increasing enzymic activities results in the phosphorylation-mediated activation or inhibition of key regulatory enzymes involved in carbohydrate and lipid metabolism. Hypoglycemia hypoglycemia can cause cerebral dysfunction, whereas severe, prolonged hypoglycemia causes brain death. It is, therefore, not surprising that the body has multiple overlapping mechanisms to prevent or correct hypoglycemia. The most important hormone changes in combating hypoglycemia are elevated glucagon and epinephrine, combined with the diminished release of insulin. Symptoms of hypoglycemia the symptoms of hypoglycemia can be divided into two categories. Adrenergic symptoms-anxiety, palpitation, tremor, and sweating- are mediated by epinephrine release regulated by the hypothalamus in response to hypoglycemia. Usually adrenergic symptoms (that is, symptoms mediated by elevated epinephrine) occur when blood glucose levels fall abruptly. Neuroglycopenia-the impaired delivery of glucose to the brain-results in impairment of brain function, causing headache, confusion, slurred speech, seizures, coma, and death. Neuro glycopenic symptoms often result from a gradual decline in blood glucose, often to levels below 40 mg/dl. Glucoregulatory systems Humans have two overlapping glucose-regulating systems that are activated by hypoglycemia: 1) the islets of Langerhans, which release glucagon; and 2) receptors in the hypothalamus, which respond to abnormally low concentrations of blood glucose. Glucagon and epinephrine: Hypoglycemia is combatted by 1 Patients with type 1 diabetes were injected with insulin. Glucagon (2 mg subcutaneous) Blood glucose (mg/dl) 40 240 Glucagon Insulin 160 decreased release of insulin and increased secretion of glucagon, epinephrine, cortisol, and growth hormone (see Figure 23. Glucagon and epinephrine are most important in the acute, shortterm regulation of blood glucose levels. Epinephrine promotes glycogenolysis and lipolysis, inhibits insulin secretion, and inhibits the insulin-mediated uptake of glucose by peripheral tissues. Epinephrine is not normally essential in combating hypoglycemia, but it can assume a critical role when glucagon secretion is deficient, for example, in the late stages of type 1 (formerly called insulin-dependent) diabetes mellitus (see p. The prevention or correction of hypoglycemia fails when the secretion of both glucagon and epinephrine is deficient. Cortisol and growth hormone: these hormones are less impor- tant in the short-term maintenance of blood glucose concentrations. Types of hypoglycemia Hypoglycemia may be divided into three types: 1) insulin-induced; 2) postprandial (sometimes called reactive hypoglycemia); and 3) fasting hypoglycemia. Insulin-induced hypoglycemia: Hypoglycemia occurs frequently in 0 0 1 2 3 4 Hours Saline 5 6 7 8 2 Some patients treated with saline instead of glucagon. Mild hypoglycemia in fully conscious patients is treated by oral administration of carbohydrate. More commonly, patients with hypoglycemia are unconscious or have lost the ability to coordinate swallowing. In these cases, glucagon, administered subcutaneously or intramuscularly, is the treatment of choice (Figure 23. It is caused by an exaggerated insulin release following a meal, prompting transient hypoglycemia with mild adrenergic symptoms. The only treatment usually required is that the patient eat frequent small meals rather than the usual three large meals.
Generic nicotinell 52.5 mg without a prescription. What Causes Chest Pain When It's Not Your Heart.